|
|
NB: the contents of this page are extracted from the original project approved by the EU in 2004.
Objectives
- The general objective of the project was:
-
to build a common European infrastructure for standardized information exchange in diabetes care, for the purpose of monitoring,
updating and disseminating evidence on the application and clinical effectiveness of best practice guidelines on a regular basis
- To fulfill the general objective, we proposed aplan based on the following rationale:
- adoption of a systems approach to make best use of different sources of information
- promotion of an efficient use of available resources, using systems already in place at the regional level
- implementation of technical solutions to build comprehensive reports on a range of outcomes
- These principles underpinned our logic for “Best Information through Regional Outcomes” (BIRO).
- The general objective has been pursued through the realization of the following specific objectives:
-
- identification of a set of clinical guidelines based on the scientific literature
- selection of a European minimum dataset for international comparisons
- adoption of common Health and Quality Indicators for routine monitoring of diabetes outcomes
- finalisation of a concept and data dictionary for information exchange and data processing
- definition of standardized statistical analyses, in the form of report templates
- design and implementation of a relational data model
- design and implementation of statistical methods for the production of health reports
- validation of a secure protocol for international communication and shared data analysis
- customisation and development of specialized software to be deployed in the public domain
- linkage of the different components in a user-friendly reporting facility
- dissemination of all results through a web portal and a specialized publication
-
Each of these objectives was made relative to a specific workpackage, presented in detail in the methodological/workplan section.
The different components together constituted a coherent system that was progressively built through the project collaboration.
-
This system was defined as “Shared EuropeanDiabetes Information System”,hereafter referred to as “SEDIS”.
The concept of SEDIS represented an efficient and sustainable solution to perform the following tasks:
-
- analysis of longitudinal trends and average outcomes in a diabetic population
- identification of patterns of care and prevention consistently showing positive results
- identification of population strata and/or practices that do not show effective results
- verification of the application/applicability of best practice guidelines
- on-field testing of collaborative information systems in chronic diseases
- Outputs of this proposal supported improved information at both the
micro and the macro levels: they will facilitate activities for
planning and management of diabetes care in regional health systems, delivering European institutions information directly applicable at the Community level.
The project exploited the following leverage points:
-
- multidisciplinary collaboration
- protection of data ownership
- privacy protection
- shared information infrastructure
- high level database and statistical technology
- software publicly available
-
Disease management is frequently represented as a quality improvement cycle, which incorporates changes from emerging best practice through
the adoption of a systematic and comprehensive evaluation model.State-of-the-art disease management programs are characterized by: 1) a
population-based systems approach; 2) proactive contacts and reminders; 3) patient-centred care; 4) accurate follow-up; 5) multidisciplinary
teams; 6) focus on outcomes and outcomes-related processes; and 7) clinical information systems to improve quality of care.
-
The availability of a system that has the ability to conduct rapid disease management evaluation at the European level is a valuable opportunity
that will be properly tested in a critical area for chronic diseases and risk prevention such as diabetes. It is fundamental that the adoption of
the disease management scheme is accompanied by clear and robust procedures for data exchange, whose structure we wish to define with accuracy in
this project. The system that we propose to build, SEDIS, will operate on top of databases already available, in a way that could provide users with
reliable information relative to: a) common patient management strategies, as expressed by agreed clinical guidelines, b) current average for the target
patient categories in the particular geographical and social context; and c) measures of ‘global variability' in diabetes care in Europe.
Previous EU Projects
-
The BIRO project was the logical continuation of a series of international projects spanning over a timeframe of more than 20 years
of research and development in diabetes care, prevention and information technology.
-
Partners of the Consortium were core activists in the implementation of the “St.Vincent Declaration” [34], a cooperative initiative
of the European Region of the International Diabetes Federation and the WHO Regional Office for Europe for the improvement of Quality of Diabetes Care,
as well as active members of the DIABCARE Q-NET project sponsored under the 4th Framework and the DIABCARD Dataset repository.
-
DIABCARE represented a breakthrough in the collection of prospective data on diabetes care. Among various innovations, the
project proposed and implemented a solution to send medical records from a range of clinical organizations to a centralised server with
storage and analysis capabilities. After many years from the completion of DIABCARE, BIRO revamped its basic intuition, improving its design with new
technology through which the management of individual records was left to the single participating institution. At the same time, BIRO showed to be substantially
stronger as it allowed delivering an in-depth analysis of systems of care, through the application of sophisticated epidemiological techniques and
advanced statistical methods that were overseen by previous projects.
-
The presentation of BIRO was also very timely as it occurred immediately after the completion of the EUDIP project. The EUDIP collaboration released
a report including a comprehensive list of quality and outcome indicators for both Type 1 and Type 2 diabetes, ranging from risk factors to process and outcome
indicators. Such measures provided an essential starting point for the construction of a knowledge repository that could be linked to records
from regional registries to drive the consequent statistical analysis of longitudinal data.
-
BIRO marked a significant step forward in the direction of identifying a final solution to monitor quality of care and outcomes in
diabetes across Europe. A key deliverable for the entire BIRO project was the provision of security mechanisms to cover all aspects of the effective
use and management of the European technical standards for data capture and transmission.
Planned Results of the BIRO collaboration
-
The project built a common infrastructure to optimize efforts in data processing and maximize outputs in terms of using evidence in the context of
modern health services delivery.
-
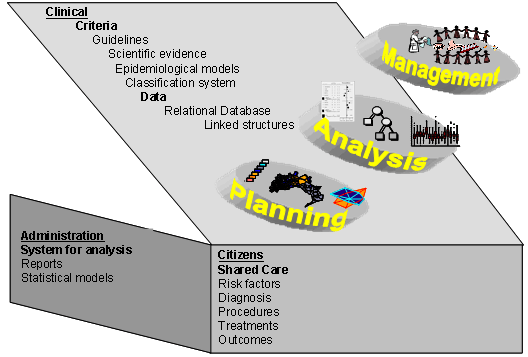
The resulting Shared European Diabetes Information System (SEDIS) was capable of delivering outputs fordifferent levels, as shown by this figure:
-
SEDIS offered value to health services organizations, policy-makers, and European citizens. The two main
technical components of the system, the Concept and Data Dictionary and the Intranet Statistical System, have
represented unique sources for the definition of standardized measuring and update of diabetes indicators.
-
The “Concept and Data Dictionary” will be available online to include information on:
-
Clinical guidelines for diabetes care
-
Clinical algorithms
-
State-of-the art epidemiological risk models
-
A concept dictionary including details on international classification systems
-
Policy algorithms as derived from regional and national regulations.
-
The “Intranet Statistical System” included advanced database and statistical routines that could be applied directly to
a regional data-warehouse, so that any region complying with the common dataset format could directly feed aggregated data to the system.
The system could produce standard reports for both the local registers and the global collaboration. Extendibility and reusability of the
product was made possible through the use of open source software.
-
Clearly, the most directly usable product of this project is the availability of reports based on very detailed diabetes data from different
parts of Europe. Such information provides the EU with a golden opportunity to investigate the impact of population characteristics (demographics,
socioeconomic, disadvantage, etc.), health care organization (settings of care, workforce), process data (health services) and outcomes (multidimensional
individual measurements) on longitudinal trends. By linking the WHO DiabCare (EU program), the Healthgate (Austria-Germany quality management project)
and the Black Sea Tele Diab (Romania program), BIRO offered results from a prospective database of more than 100,000 patients, allowing for the first
time the comparison between data of EU/EFTA/AS countries. All partners had strong links with research centres and companies outside the Consortium,
making the continuous expansion of the BIRO network possible.
Future use of the Shared Information System
-
This model could offer direct advantages to many potential users in the European Union interested in better information from three different
perspectives (see figure above): governance, disease management and systems modelling.
-
Clinical governance is a relatively recent concept that has influenced the organization of modern health systems and consequently
could play a role in shaping the future solutions for high priorities as diabetes [37]. The concept advocates an efficient use of resources on the basis of population
needs, to support the adoption of adequate prevention strategies and health services based on the evidence and the actual health needs. In
other terms, governance analysis concerns the balance between an optimal plan and utilization of health services to cover population
health needs [38-42]. The concept is intimately related to the principle of accountability, which is in turn only possible through the
availability of up-to-date, well structured information.
-
This condition, except for few successful examples [43], has been rarely realized at a health system level worldwide, and it is certainly a long
term perspective at the level of the European Community. Nonetheless, SEDIS allowed making significant progress in this direction, providing
tools for accurate benchmarking that at the time certainly did not exist. The system that we proposed allowed answering very rapidly to questions such as:
what is the average difference in glycated haemoglobin that a system can achieve within six months, with this therapy, in similar
conditions? What is the average length of stay for a particular procedure? What outcomes can clinicians achieve for this particular
population of patients? Why countries experience such large variations? Why these outcomes are so different between countries? These aspects
are important to both realise global accountability as well as informing local practitioners and, through them, the citizens.
-
The characteristic linkage of SEDIS (and thus of EU health reports) to regional registers provided the means to pass on this information
through disease management programs running on a daily basis. In other words, differently from other projects for health policy, the results
of BIRO linked directly to everyday practice. Disease management is the key instrument that was targeted to support the continued availability of such
information. The cycle was virtuous as it could generate synergies resulting in improved health outcomes for the patients. Managed care
organisations that consistently monitor quality were showing significant improvements in outcomes, even short term, particularly because such information
could support a more intensive follow up that could be effective in treating many different conditions [44-48]. The BIRO project, with its characteristic
plan supporting participation and dissemination, can advance previous European experiences in the field made by continental projects [1-49].
SEDIS was designed to provide a stronger basis for outcomes of disease management strategies, an integral part of the organization of regional activities [3-8,46-47]
in which all partners of the BIRO Consortium were consistently involved with.
-
BIRO has developed modelling functionalities that were usually never included in health information systems. Such feature
was extremely relevant for the dissemination of our product, as it attracted the interest of many potential new users. The online availability of
specialized software that could freely downloaded represented an ideal springboard for further development. A specific target of SEDIS was the development of
multivariate models [50-51] that were needed to overcome the limitation of traditional approaches [29]. The availability of foundations work offered
new opportunities for better and more robust health systems analysis [52-54].
Public software for the e.health landscape
-
The innovative aspects of SEDIS facilitated the integration of its design with a range of innovative e.health projects.
The development of health information systems is crucial to create new interfaces between
end-users and the community of health practitioners. Despite the high priority of diabetes, there
were scarce opportunity for citizens to interact with their own
clinicians having a clear idea of the best achievable targets applicable to their conditions.
-
The development of a common framework created new chances to operate in this direction, since reports were designed to be publicly available on
our website. While the statistical design of SEDIS built upon previous research projects experiences of research projects [55-57], its
large scale implementation paved the way for using the same approach in other situations. To this end, using open source programming languages [59]
represented a strategic element to combine European policy objectives with relatively low-cost solutions.
|
